Heart
The heart (lat. cor) is a hollow muscle. Through its contractions the blood is pumped through the body. It is a vital organ that ensures the necessary supply of blood to the other organs.
Heart in situ
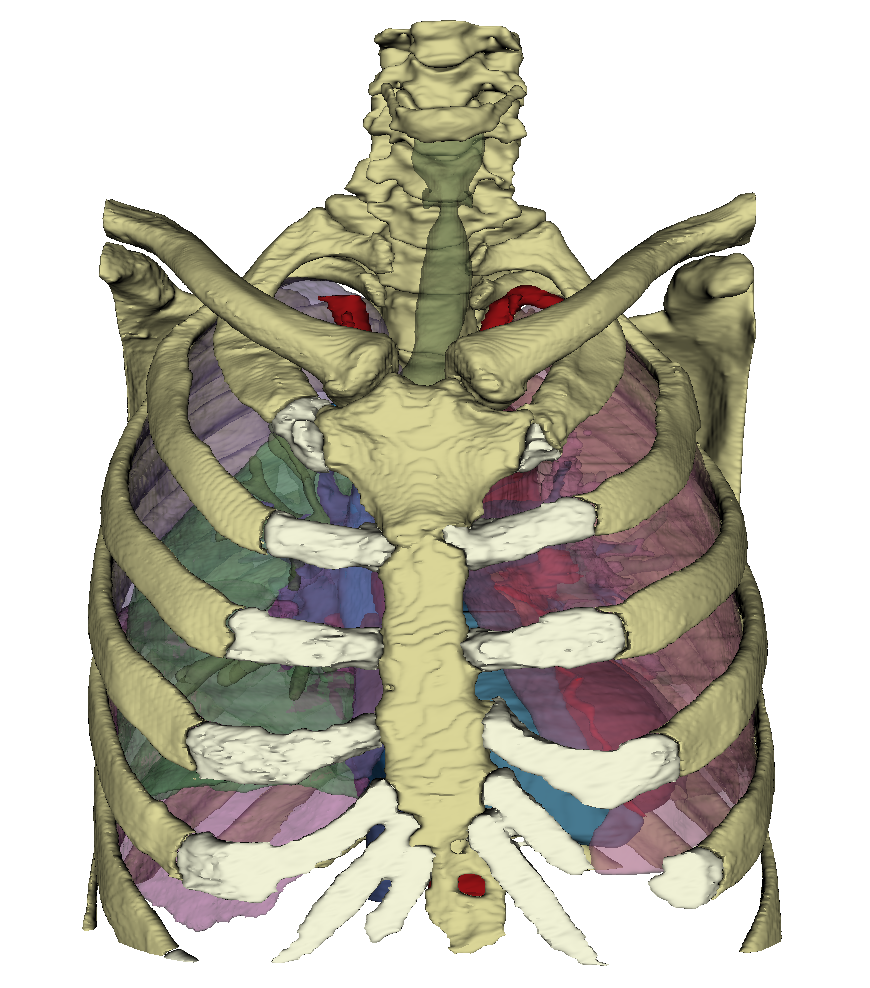
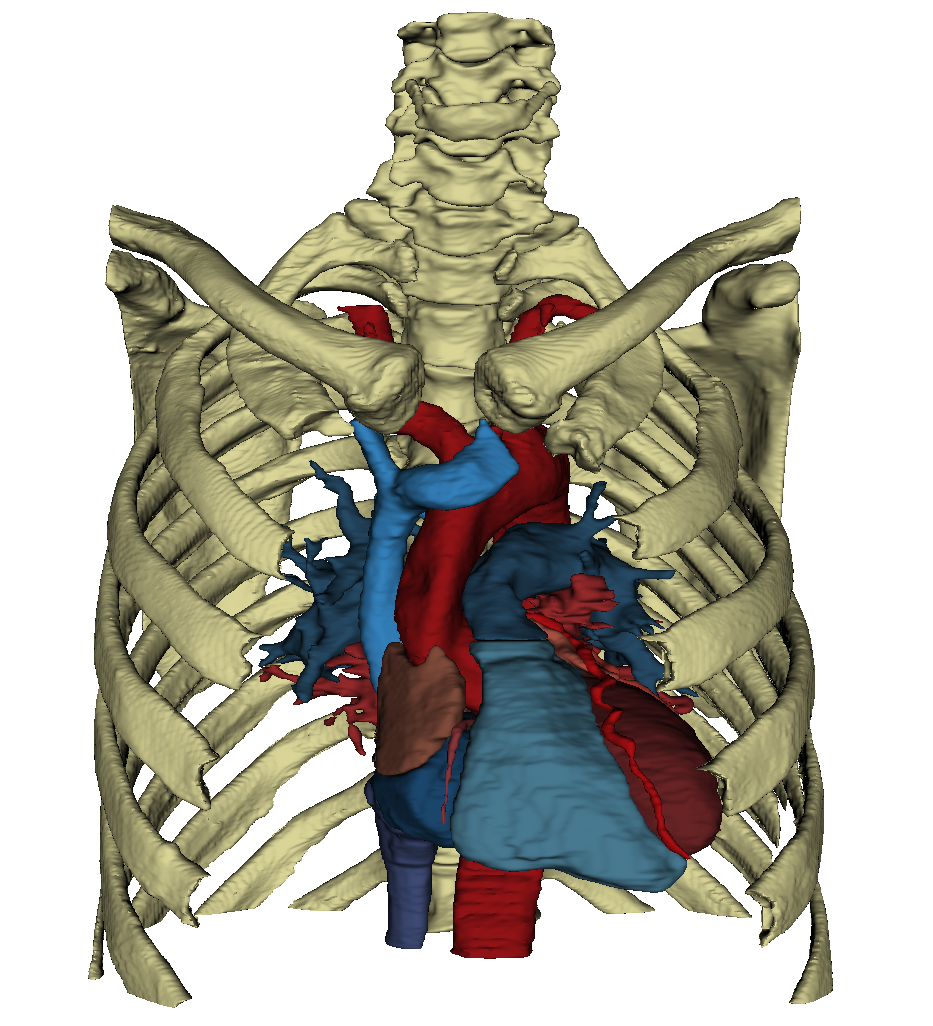
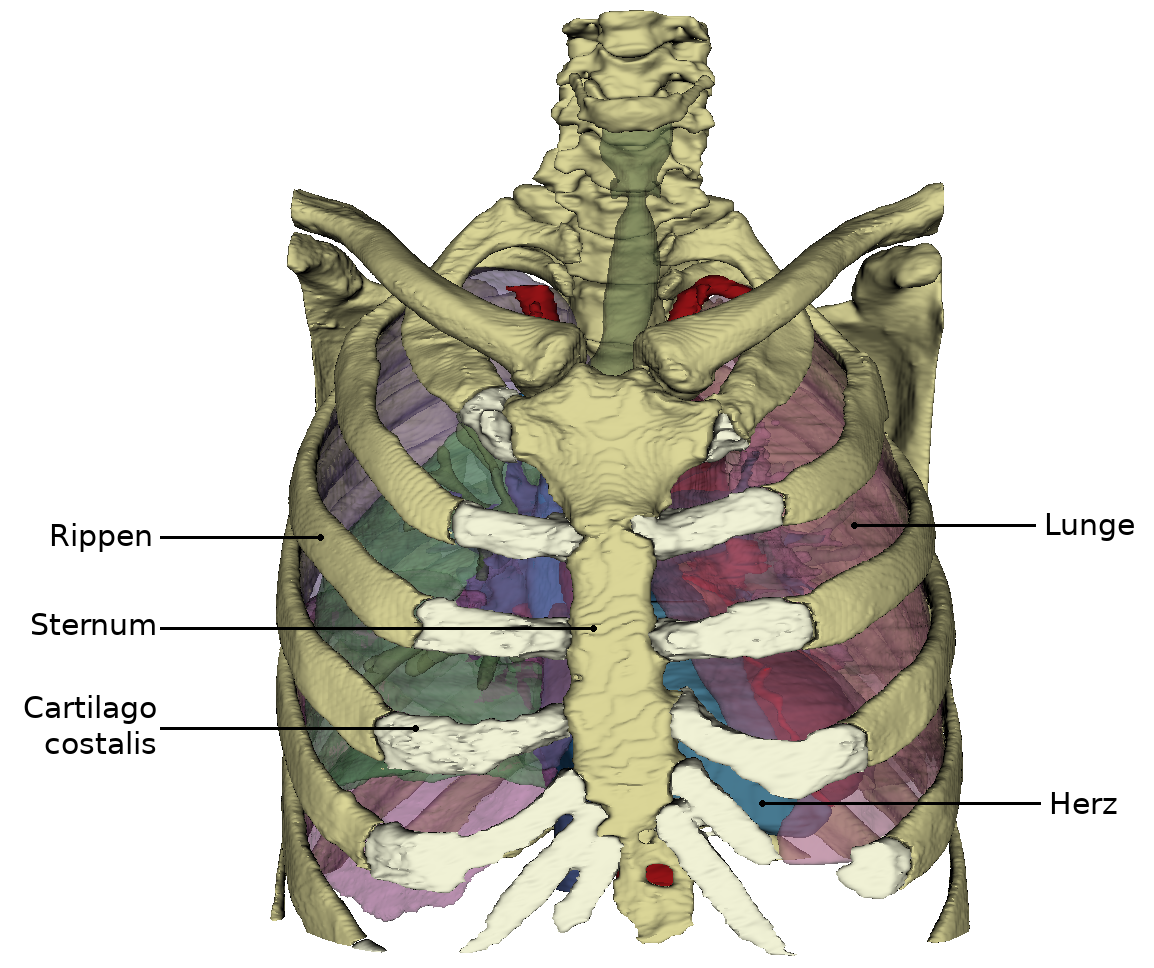
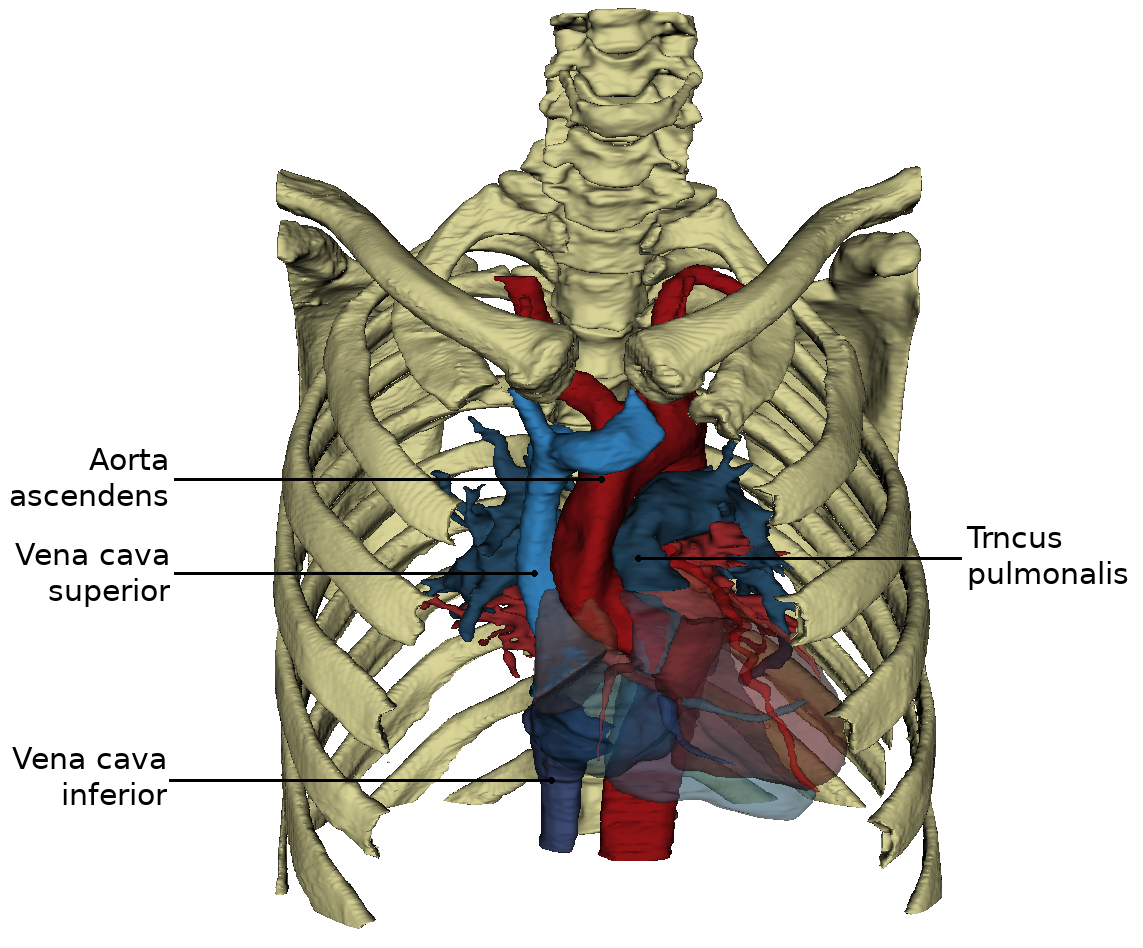
The heart is located approximately in the middle of the thorax, which is called the mediastinum. The representation in the WebViewer is greatly simplified. In order to have a clear view of the heart, the thorax must be opened extensively and the connective tissue in the mediastinum anterius removed. Approximately two-thirds of the heart is located to the left of the breastbone and one-third to the right. The apex of the heart (apex cortis) points to the left front and lies on one level with the left nipple. Its contraction (the so-called cardiac apex thrust) can be felt as a tender beat through the chest wall. Viewed ventrally, the heart is located obliquely and turned counterclockwise in the thorax. At the front it reaches the sternum and at the back it is bounded by the trachea and oesophagus. On the left and right it is surrounded by the lungs. The right ventricle is clearly visible from the ventral view. The left ventricle is only partially visible. Even the large vessels are not all visible at the base of the heart. The vv. pulmonales lies on the flip side of the heart and merges in the left atrium, which is also dorsal. Clearly recognizable, however, are the two heart ears (auricula sinistra and dextra), each located on the periphery.
Form and structure










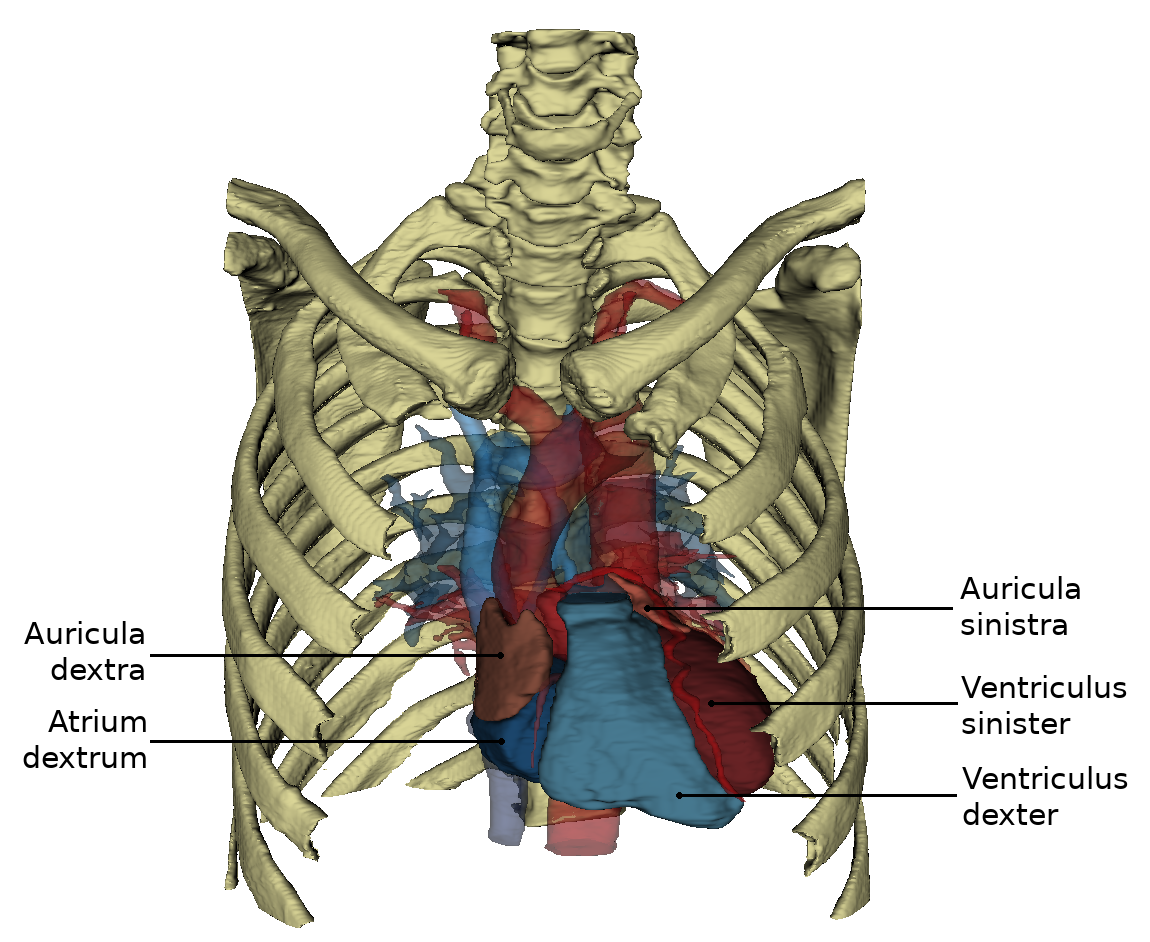
View from ventral
The heart (Cor) has the shape of an obliquely inclined cone and is a muscular hollow organ.
The following structures are differentiated in the heart:
- a downward, left and ventrally inclined tip of the heart,
- three areas, whose names are mostly based on the adjacent thorax walls
- a heart base inclined upwards, to the right and dorsally
On the side of the heart that rests on the sternum and costae, you can see the right ventricle, which is separated from the left ventricle by the sulcus interventricularis anterior. From this angle, the left ventricle forms the left edge of the heart and the apex cordis.
The anterior interventricular groove (sulcus interventricularis anterior) contains the r. interventricularis anterior of the a. coronaria sinistra and the v. interventricularis anterior. The sulcus interventricularis anterior describes the course of the ventricular septum inside the heart.
The atria (atrium sinistrum and dextrum) are separated from the ventricles by the sulcus coronarius, which also contains coronary vessels.
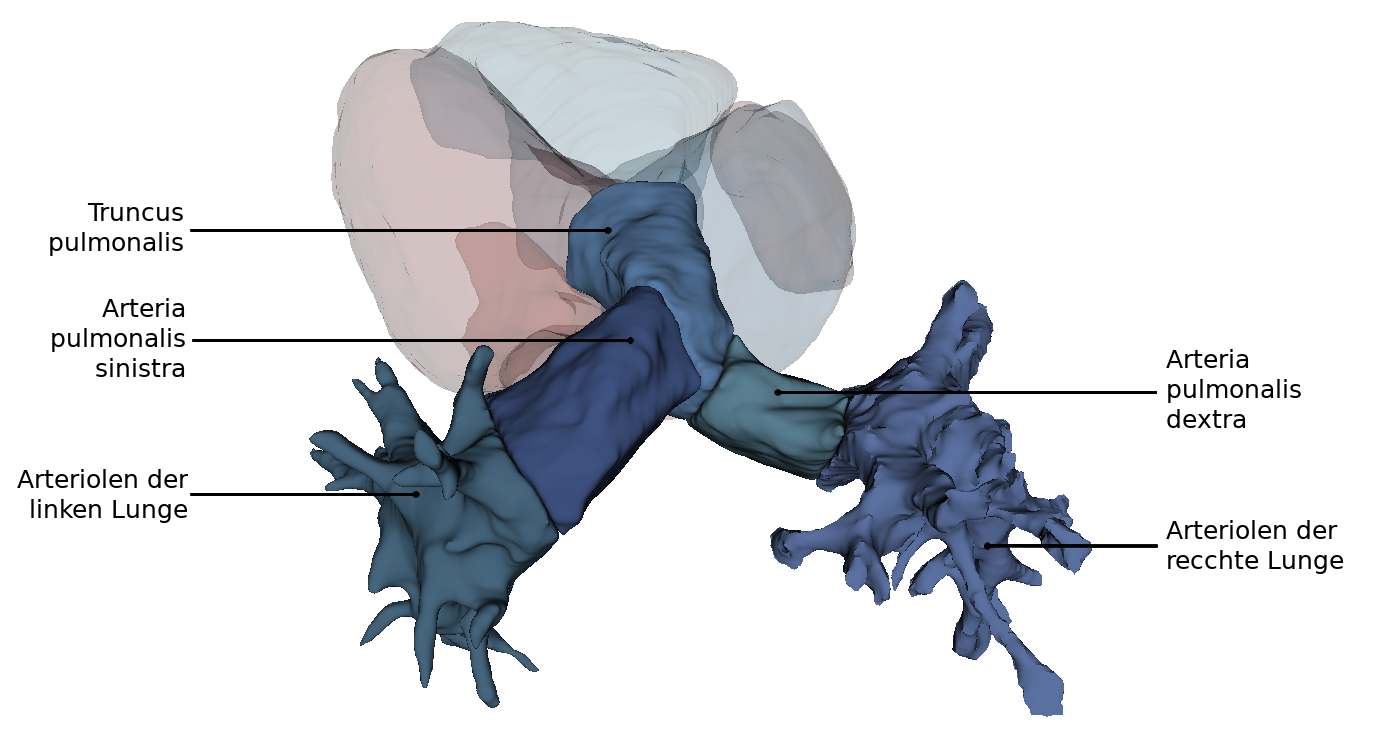
The right atrium (auricle dextra) attaches to the base of the aorta (pars ascendens), the left atrium (auricle sinistra) to the base of the truncus pulmonalis. From this perspective, the aorta obscures the exit of the right pulmonary artery from the pulmonary trunk.
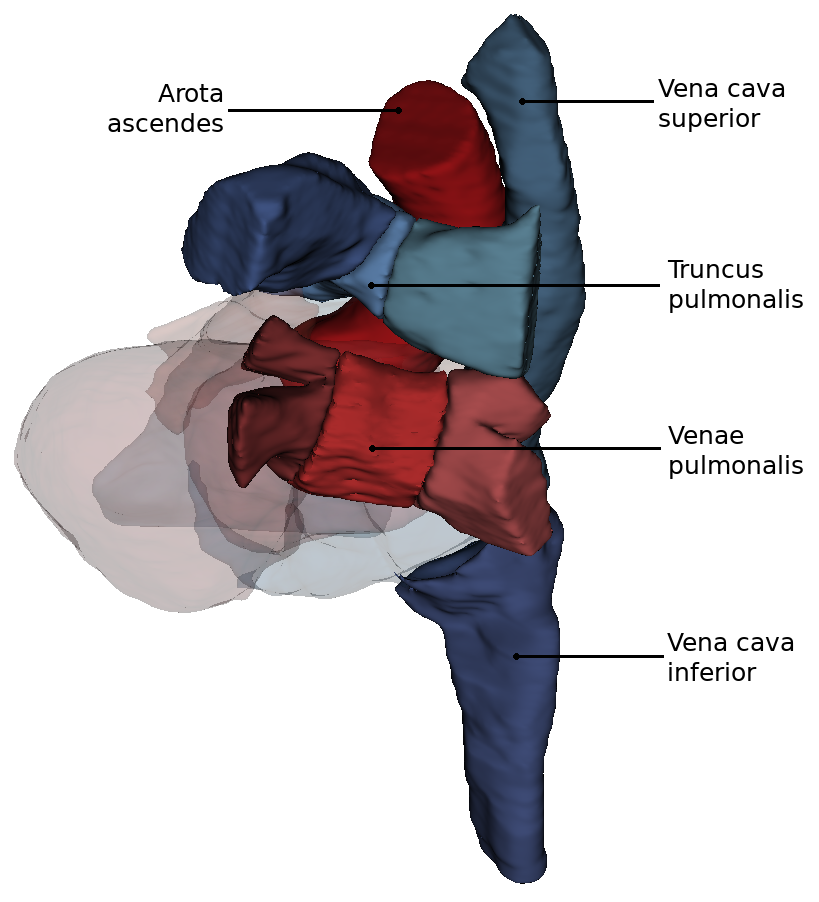
View from dorsal and caudal
By turning the heart ventrally, the side facing the diaphragm (Fascies diaphragmatica) becomes more visible. Exclusively from caudally from the viewing direction of the diaphragm it can be seen that the both Vv. cavae lie in one axis.
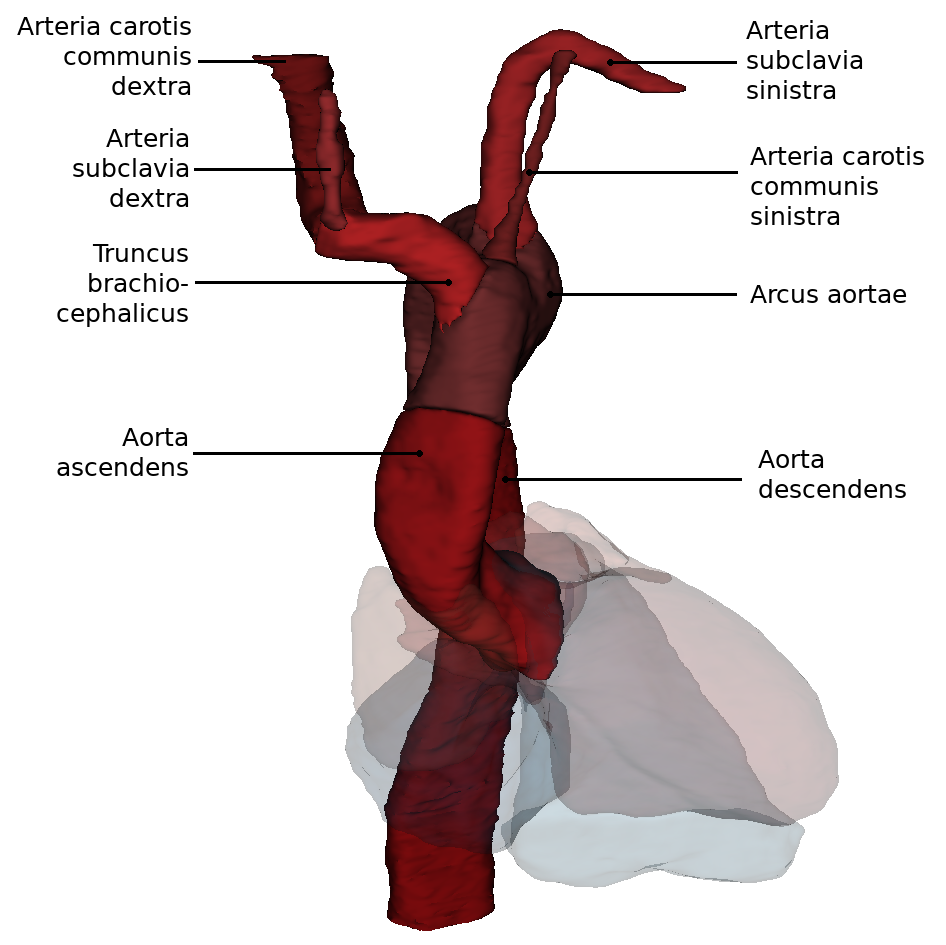
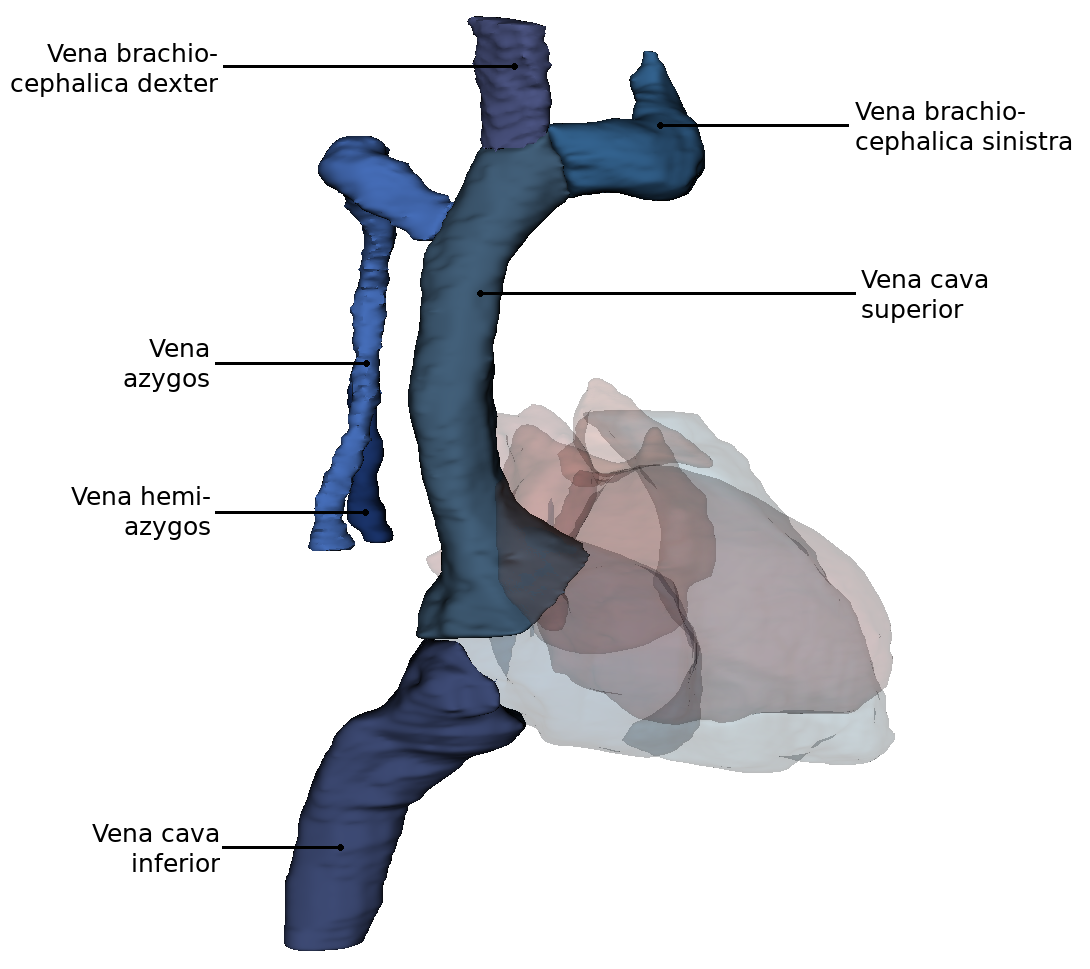
View from dorsal
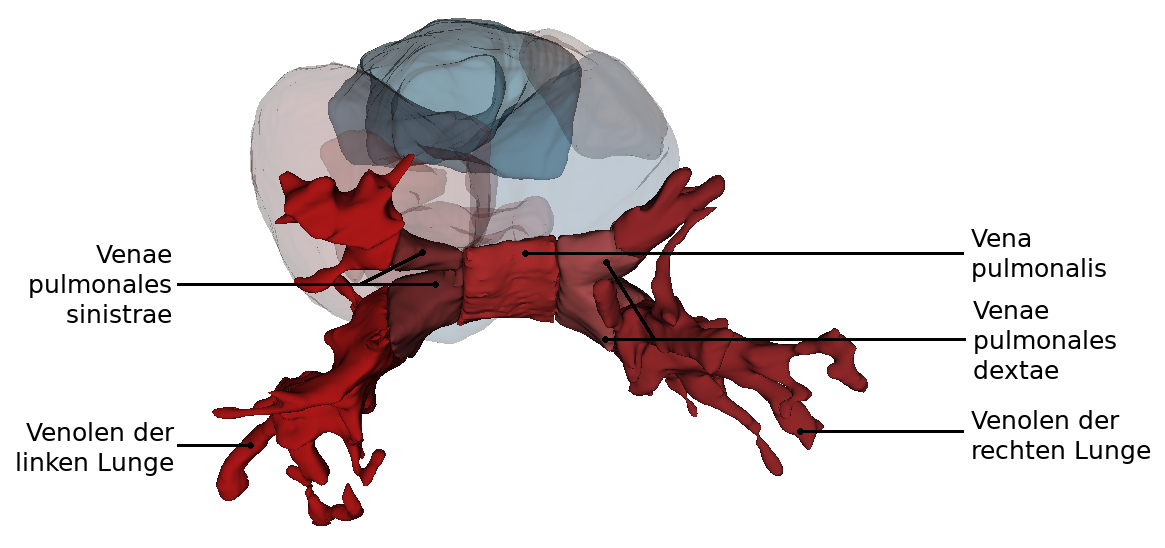
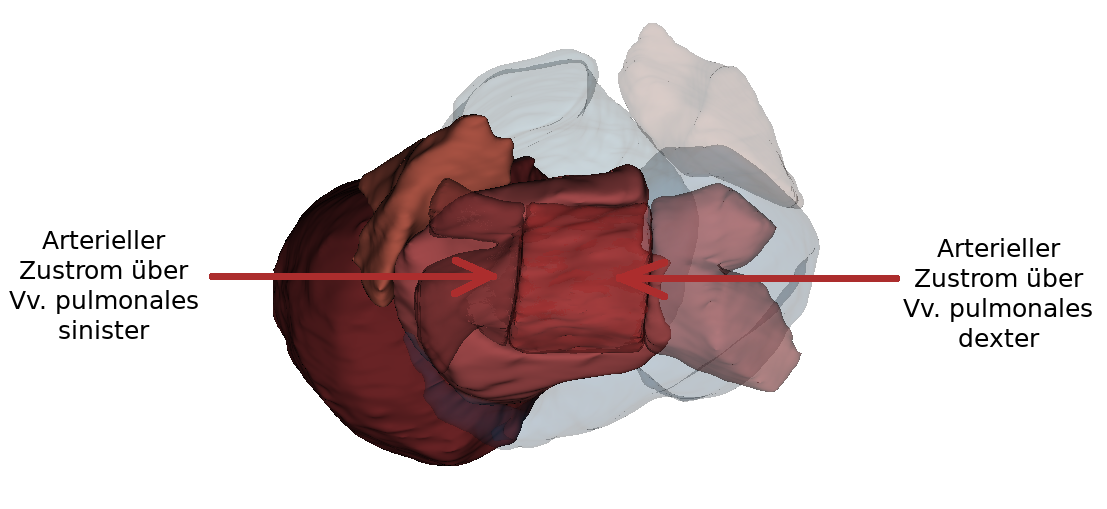
From this perspectiveit is clearly visible how the Arcus aortae crosses the Truncus pulmonalis, where it divides into the A. pulmonalis sinistra and A. pulmonalis dextra. At this point the three major arteries branch off to the upper extremity and to the neck and skull: Truncus brachiocephalicus, A. carotis communis sinisra and A. subclavia sinistra. Also the orifices of the - usually four - Vv. pulmonales into the left atrium (Atrium sinistrum) and the two Vv. cavae into the right atrium (Atrium dextrum) are well visible. Also visible here is the sinus coronarius in the sulcus of the same name. This sinus is the collection vessel for the venous blood that is supplied to the heart via the Vv. cardiacae.
Inner spaces
In the heart, four internal spaces are distinguished (one chamber (ventricle) and one atrium (atrium) on the left and right respectively). The atria are adjacent to the ventricles, which are connected to the lungs or the major arteries and veins of the body by their outgoing vessels.
Inner spaces of the left heart
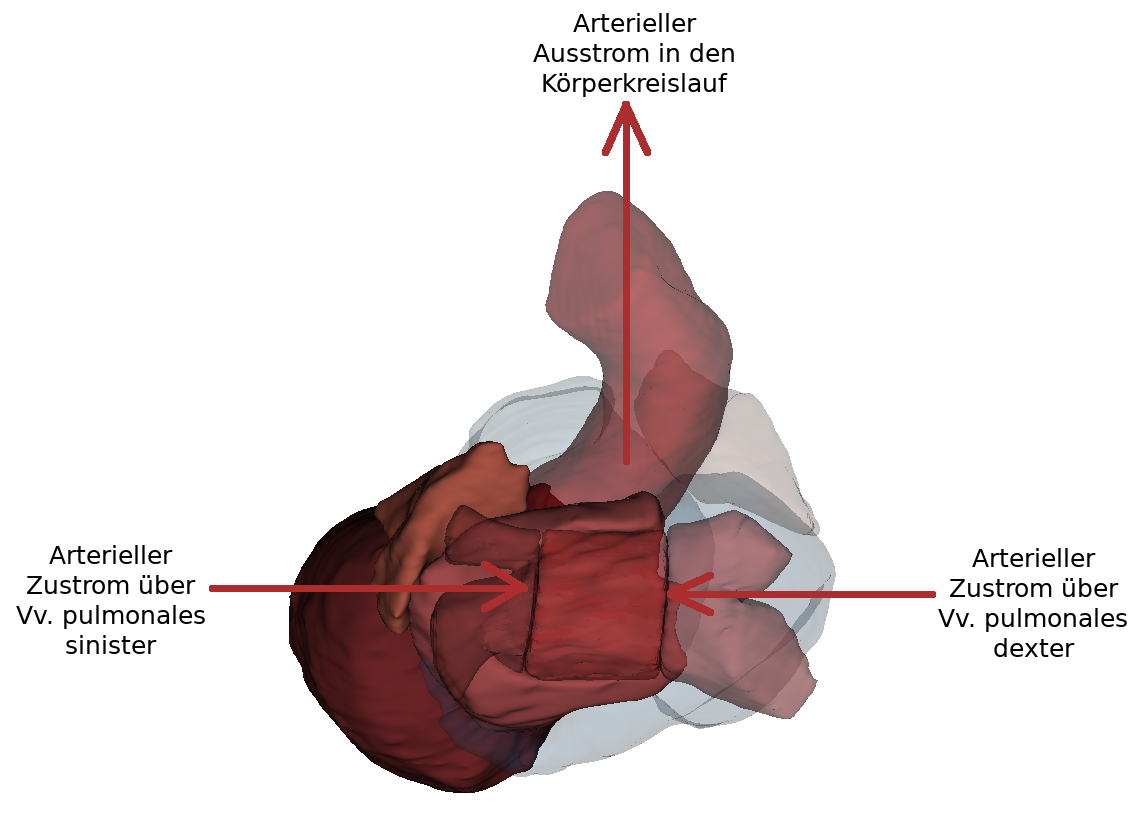
The left atrium has smooth walls between the openings of the four pulmonary veins (Vv. pulmonales dextra/sinistra superior and inferior). The muscle wall of the left atrium is thinner than that of the right atrium because it belongs to the low pressure system. The narrow fold (valvula foraminis ovalis) is temporarily visible at the septum interatriale. It is formed by raising the fossa ovalis into the left atrium.
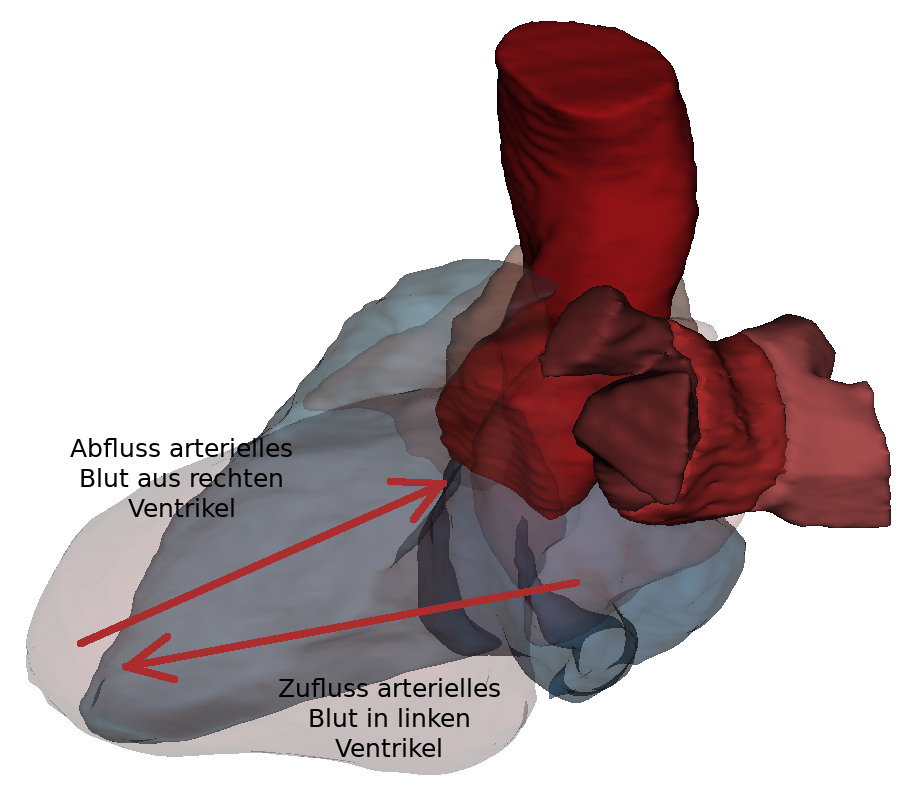
Blood passes from the left atrium into the left ventricle via the ostium atrioventriculare sinistrum.. The ostium atrioventriculare can be closed by the valva atrioventricularis sinistra. The left ventricle also has an inflow and outflow pathway. The inflow passes along the posterior wall, the left lateral wall as well as the apical section. The smooth-walled outflow tract is located near the septum interventriculare and continues into the vestibulum aortae. It consists largely of musculature (pars muscularis). The ostium aortae is the opening between the aortic outflow tract of the left ventricle and the aorta. The wall of the left ventricle is about three times as thick as that of the right ventricle and thus belongs to the high-pressure system.
Inner spaces of the right heart
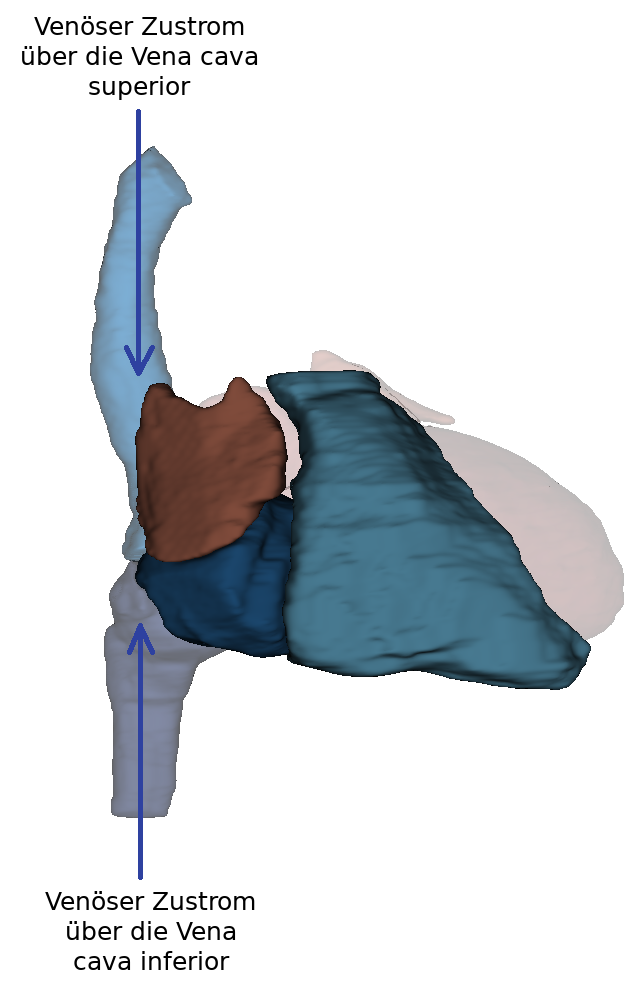
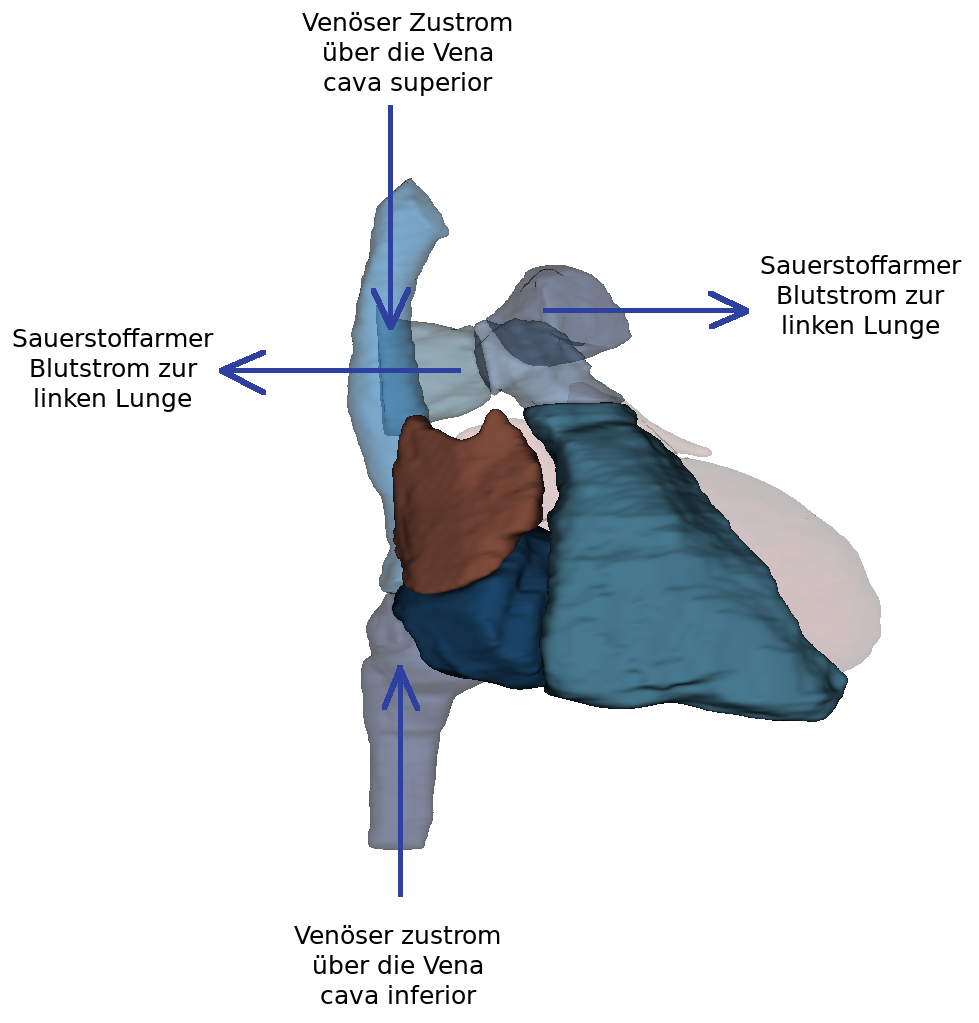
The posterior part of the right atrium consists of the sinus venarum cavarum (atrial sinus). At the ostium cavea superioris and inferioris the two vv. cavae (superior and inferior) open. From these, blood can flow seamlessly into the atrium without intervening valves. The oval fossa is located above the confluence of the inferior vena cava and is surrounded by the oval fossa limbus. The crista terminalis separates the anterior part (right atrium with heart ear) from the posterior.
The right atrium is larger than the left and also belongs to the low-pressure system. In contrast to the smooth-walled anterior section of the atrium, the posterior part has significantly more structure.
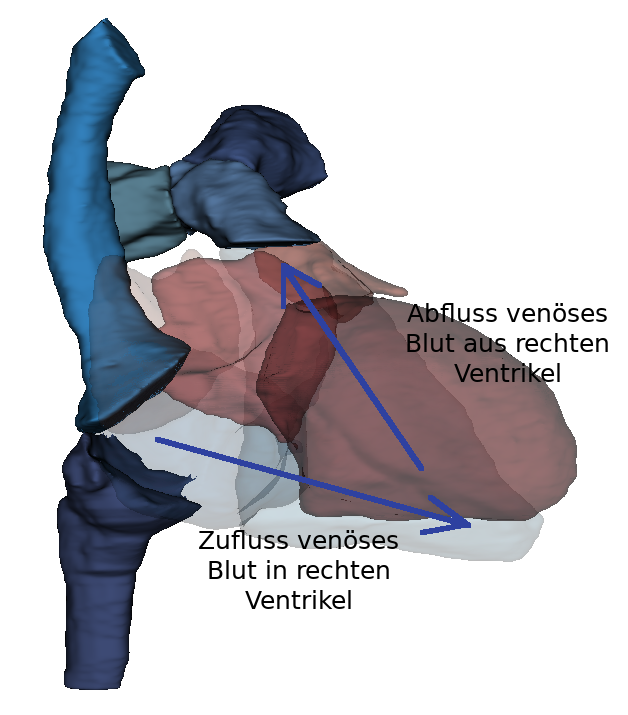
The right ventricle can also be separated into two parts by the trabeculae carnea and the crista supraventricularis.
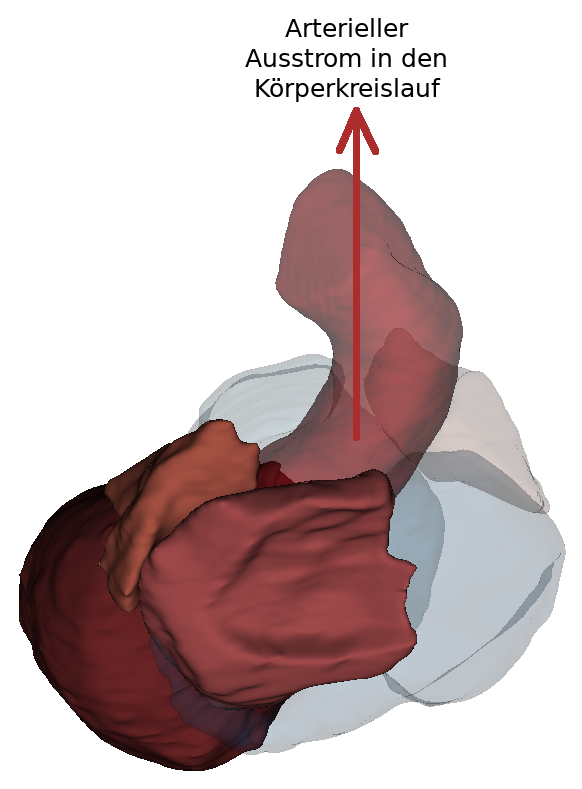
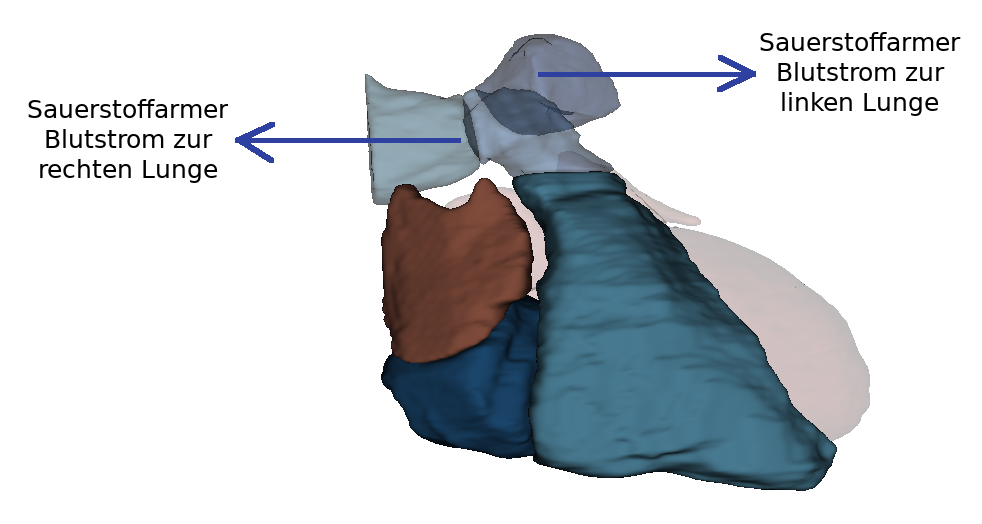
The blood flows via the ostium atrioventriculare dextrum into the right ventricle. Here, too, there is an inflow and outflow trajectory. In the inflow area are the trabeculae carneae, which are small muscle bulbs. Here too, the papillary muscles are connected to the valva atrioventricularis (dextra) via chordae tendineae. The outflow tract continues over the conus arteriosus. The conus arteriosus is the cone-shaped transition of the right ventricle into the truncus pulmonalis. This area is smooth-walled and has no trabeculae carneae. The blood flows over the pulmonary valve (valva trunci pulmonalis) through the ostium trunci pulmonalis into the truncus pulmonalis. The right ventricle also belongs to the low-pressure system.
Overview of the heart valves
There are two types of valves in the heart: atrioventricular valves and vascular valves. The four heart valves serve to allow blood to flow in the heart in only one direction and thus prevent backflow of blood. The leaflet valves are located between the atria and the ventricles. The pocket valves are located between the pulmonary trunk and the aorta.
Sail valves (Valvae atrioventriculares)
The sail valves (valvae atrioventriculares) are also called atrioventricular valves (AV valves). They include the tricuspid valve (valva atrioventricularis dextra) and the bicuspid valve (valva atrioventricularis sinistra). These valves prevent the backflow of blood from the ventricles into the atria during contraction of the heart. The name of the valves comes from their shape, which resembles a sail. They project into the ostium atrioventricularis dextrum as well as sinistrum. The sail valves are attached to the musculi papillares via the chordae tendinae. These are a special form of the trabeculae carneae. Thus, the leaflet valves are mechanically attached to the cardiac skeleton.
During systole, the blood is forced out of the ventricle. In the process, the leaflet valves inflate and are filled with blood. The anchoring of the valves to the chordae tendinae and the contraction of the papillary muscles prevent the valves from opening into the atrium. The leaflet valves are located at the level of the ostium because the bulging of the leaflets towards the atrium is cancelled by the retraction of the papillary muscles.
Tricuspid valve
The tricuspid valve is located between the right atrium and ventricle. It prevents systolic backflow of blood from the right ventricle into the right atrium. It is made up of three leaflets: Cuspis anterior, cuspus posterior and cuspus septalis.
Bicuspid valve
The bicuspid valve is located between the left atrium and the left ventricle. Unlike the tricuspid valve, the bicuspid valve consists of only two leaflets (cuspis anterior and cuspis posterior).
Semilunar valves (Valvae semilunares)
The pulmonary valve and the aortic valve belong to the semilunar valves. Their structure is made up of a thin connective tissue with an endocardial covering. The valves are composed of three crescent-shaped pockets (valvula semilunaris anterior, sinistra and dextra) and open in the direction of the vessels in the ostium aortae or ostium trunci pulmonalis. The individual valves have a free edge (lunula valvae semilunares), which thickens in the middle to form a small connective tissue nodule (nodulus valvulae semilunaris). When the valve closes, the nodules and lunulae meet. In this way, the ostium is completely sealed. The backflow of blood is prevented by filling the pockets. No muscle contraction is necessary in this process.
Pulmonalklappe (Valva trunci pulmonalis)
Durch die Pulmonalklappe wird der Rückfluss des Blutes in den rechten Ventrikel verhindert. Da diese Klappe zwischen zwei Niederdrucksystemen (venöser Schenkel des Körperkreislaufsystem und Pulmonalkreislauf) ist sie dünner ausgeprägt.
Aortenklappe (Valva aortae)
Durch die Aortenklappe wird der Rückfluss aus der Aorta in den linken Ventrikel verhindert. Sie hat eine leichte Auswölbung nach außen (Sinus aortae). Die Herzkranzgefäße (A. coronaria sinistra und dextra) entspringen im linken und rechten Sinus aortae, so dass das Herz mit Blut versorgt wird.
Herzauskultation
Bei einer Funktionsstörung entstehen durch Wirbelbildungen des Blutes hörbare Strömungsgeräusche. Zur Erkennung dieser Geräusche ist die Herzauskultation eine alte, aber wichtige Methode. Sie dient sowohl der Ersterkennung als auch der Verlaufskontrolle von Funktionsstörungen. Die Grundlage ist, dass beim gesunden, erwachsenen Herzen zwei Töne zu hören sind. Dabei ist der erste Herzton (S1) am Beginn der Systole. Erzeugt wird der Ton durch die Blutsäule, die gegen die Segelklappen schlägt und nicht, wie häufig angenommen, durch den Schluss der Klappen. Der zweite Herzton (S2) wird durch den Verschluss der Taschenklappen am Ende der Systole erzegt. Er ist im Vergleich zum ersten Herzton deutlich heller. Die beiden Töne sind an unterschiedlichen Orten deutlich zu hören. Über der Herzspitze ist der erste Herzton deutlich zu hören, über der Herzbasis dagegen der zweite Herzton. Am Erb'schen Punkt, der links parasternal im dritten Interkostalraum liegt, können alle Herzklappen gleich gut erfasst werden. Für die Auskultation einzelner Herzklappen werden bestimmte Punkte am Brustkorb empfohlen, da die geräusche an diese Orte projiziert werden und so am lautesten zu hören sind:
- Aortenklappe: 2/3. Interkostalraum rechts parasternal
- Pulmonalklappe: 2. Interkostalraum links parasternal
- Trikuspidalklappe: 4. Interkostalraum rechts parasternal
- Bikuspidalklappe: 5. Interkostalraum links medioklavikulär
Erregungsbildungs- und Erregungsleitungssystem (Demnächst)
Im Herzen gibt es ein autonomes Erregungsbildungssystem (Systema conducente cordis) und ein Erregungsleitungssystem (Systema conducente cordis). Es werden dabei vier Abschnitte unterschieden. Bei der Erregung des Herzen spannt sich die Vorhof- und Kammermuskulatur ca 100.000 Mal pro Tag. Dabei wird der Herzmuskel durch elektrische Impulse gesteuert. Die entstandenen Impulse verbreiten sich in einem speziellen Zellsystem des Herzmuskels.
Sinusknoten
Der Sinusknoten wird auch Nodus sinuatrialis oder Keith-Flack-Knoten genannt. Er besteht makroskopisch aus einer muskulären Struktur, die etwa 3 mm dick und 10 mm lang ist. Die äußere Form ähnelt einem Komma. Er befindet sich an der Dorsalseite des rechten Herzens und ist dort subepikardial im Sulcus terminalis gelegen. Kranial vom Sinusknoten befindet sich die Einmündung der Vena cava superior. In manchen Fällen reicht der Sinusknoten bis in das rechte Herzohr hinein.
Funktionell gesehen, ist der Sinusknoten das primäre Schrittmacherzentrum des Herzens und ist damit an der komplexen Regulation der Herzfrequenz beteiligt. Dem Sinusknoten fällt die zentrale Rolle der Erregungsbildung zu. Es werden durch ihn Erregungssalven mit einer Ruhefrequenz von 60-70 Impulsen pro Minute erzeugt. Die Impulse werden für eine Erregung des Vorhofmyokards genutzt, da sich die Vorhoferregungswelle in Richtung der Kammern ausbreitet. Der Ramus nodi sinuatrialis sorgt für die Durchblutung des Sinusknoten. Angesteuert wird er durch den Sympathikus und Parasympathikus. De Sinuknoten besteht aus spezifischen Herzmuskelzellen:
P-Zellen
Die P-Zellen ("Pacemaker") sind rundliche, blasse Zellen, die meistens in Gruppen vorliegen. Sie sind untereinander durch Nexus und Desmosomen verbunden.
Transitionszellen
Transitionszellen sind elongierte und teilweise verzweigte Kardiomyozyten. In diesen sind sehr viele Myofibrillen enthalten. Durch die Transitionszellen werden die P-Zellen verbunden und eine Verbindung zum Arbeitsmyokard hergestellt.
Atrioventrikularknoten
Der Atrioventrikularknoten wird auch Nodus atrioventricularis, AV-Knoten oder Aschoff-Tawara-Knoten genannt. Er ist das sekundäre Schrittmacherzentrum des Herzens. Der AV-Knoten ist 5 mm lang, 3 mm breit und 1 mm dick und ist im rechten Herzvorhof angesiedelt. Die genaue Position ist an der Basis des Vorhofseptums vor der Einmündung des Sinus coronarius. Dieser Bereich wird als Koch-Dreieck bezeichnet. Der Atrioventrikularknoten dient der Regulierung der Reizübertreibung über das nichtleitende Herzskelett. Er wird durch das His-Bündel fortgesetzt, welches in Richtung der Herzspitze weiter zieht. Angesteuert wird der AV-Knoten ebenfalls durch den Sympathikus und den Parasympathikus. Die Durchblutung findet durch den Ramus nodi atrioventricularis aus dem Arteria coronaria dextra statt. Die Hauptaufgabe liegt in der Verzögerung der Erregungsübertragung auf die Kammern. So wird sichergestellt, dass die Vorhofkontraktion abgeschlossen ist, bevor die Kammerkontraktion beginnt. Durch den AV-Knoten können auch spontane Erregungen erzeugt werden. Diese haben aber eine deutlich geringere Frequenz (40-50 Depolarisationen pro Minute) als der Sinusknoten. Diese Impuls-Erregung findet nicht statt solange der Sinusknoten intakt ist.
Atrioventrikularbündel
Das Atrioventrikularbündel, auch Fasciculus atrioventricularis, AV-Bündel oder His-Bündel, ist ein Bestandteil des Erregungsleitungssystems des Herzens. Er ist 4 mm dick und 20 mm lang. Das AV-Bündel geht subendokardial im Vorhof vom AV-Knoten aus. Es durchdringt das Trigonum fibrosum dextrum und teilt sich danach in der Pars membranacea des Ventrikelseptums in die beiden Tawara-Schenkel. Die Funktion des AV-Bündels ist die Weiterleitung der Erregung von AV-Knoten bis zu den Kammerschenkeln.
Kammerschenkel
Die Kammerschenkel werden auch als Crus dextrum und sinistrum oder Tawara-Schenkel bezeichnet. Die Tawara-Schenkel teilen sich an dem AV-Bündel. Ihre Hauptaufgabe ist die Weiterleitung der Erregung aus dem His-Bündel über das Nexus in das Arbeitsmyokard. Der linke Tawara-Schenkel (Crus sinistrum) zweigt sich so gut wie senkrecht vom His-Bündel ab und fächert sich daraufhin auf. So werden folgende Strukturen erzeut: posteriorer faszikel, mittlerer Faszikel und anteriorer Faszikel. Der rechte Tawara-Schenkel (Crus dextrum) verläuft weiter nach vorne und tritt in das Myokard des Kammerseptums ein. Er verläuft weiter in Richtung Herzspitze. Im Kammermyokard wird die Erregung über die Purkinje Fasern weitergeleitet.
Erkrankungen
Freies Explorieren
- Herz
- Herzgefäße
- Binnenräume im Herz
- Herz in situ
Schauen Sie sich das Herz in 3D an und explorieren Sie sie frei. Danach können Sie sich andere Fälle ansehen oder Ihr erlerntes Wissen durch die Übungsaufgaben überprüfen.
Schauen Sie sich die Gefäße an, welche das Herz mit dem Körper und Lungenkreislauf verbinden sowie einige Herzkranzgefäße.
Betrachten Sie die Binnenräume in den einzelnen Teilen des Herz.
Betrachten Sie das Herz in situ.